Detection of early esophageal neoplastic lesions by quantitative fluorescence molecular endoscopy using oral administration of bevacizumab-800CW and cetuximab-800CW

Abstract
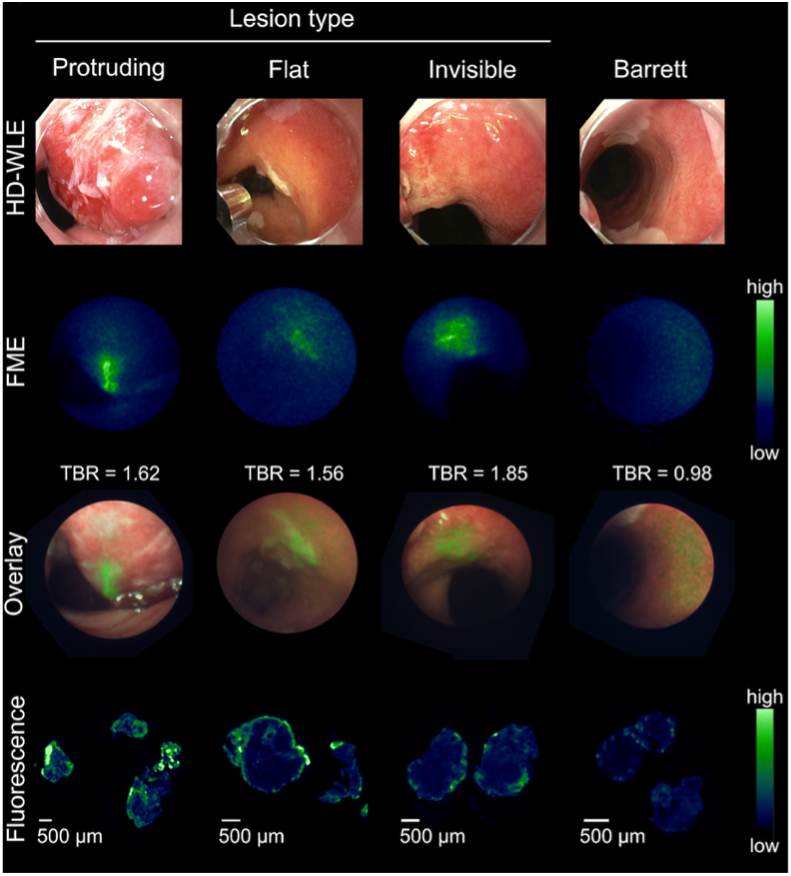
Patients with Barrett’s esophagus (BE) have an increased risk of developing esophageal adenocarcinoma (EAC) and therefore surveillance is necessary. However, lesion detection with only high-definition white light endoscopy (HD-WLE) with narrow-band imaging (NBI) has major limitations. For this reason, several different imaging modalities have been developed over the past few years. Optical molecular imaging of neoplasia associated biomarkers showed to be beneficial in lesion detection. Our research group developed a fluorescent tracer by labeling the humanized monoclonal antibody bevacizumab, targeting vascular endothelial growth factor A (VEGFA), with a fluorescent dye 800CW. The VICE study showed that synchronal use of VEGFA-guided quantitative fluorescence molecular endoscopy (qFME) and HD-WLE with NBI could improve early lesion detection by 33% using the topically applied tracer approach compared to standard HD-WLE/NBI endoscopy (1). qFME with topical administration of bevacizumab-800CW was further validated in sixty patients within the follow-up ESCEND study (unpublished data). Similar results were observed regarding lesion detection with qFME compared to the standard HD-WLE/NBI performed by the BE-expert endoscopist. When comparing this technique to a non-BE expert endoscopist even a bigger increase in lesion detection was realized. Additionally, two other tracers were investigated in a subset of 20 paired patients, cetuximab-800CW, targeting epidermal growth factor receptor (EGFR) and the nonspecific near-infrared fluorescent dye indocyanine green (ICG). qFME with cetuximab-800CW detected 17 lesions compared to 12 lesions detected by HD-WLE/NBI performed by the BE expert endoscopist (+42%) and 9 lesions detected by the non-BE expert endoscopist (+89%) (2). How different lesion types are detected by qFME with cetuximab-800CW is shown in Figure 1. These studies confirmed the great potential of qFME with targeted tracer administration for lesion detection in BE. However, by topical administration of the tracer, the procedure time is prolonged due to the five-minute incubation time. Therefore, within the SLURP study optimized oral tracer administration is evaluated to shorten the procedure time. Furthermore, simultaneous use of two tracers targeting the heterogenous expression of VEGFA and EGFR will be investigated for the detection of EAC. Thus far seven patients have been included.
References
- Nagengast WB, Hartmans E, Garcia-Allende PB, Peters FTM, Linssen MD, Koch M, Koller M, et al. Near-infrared fluorescence molecular endoscopy detects dysplastic oesophageal lesions using topical and systemic tracer of vascular endothelial growth factor A. Gut. 2019 Jan;68(1):7-10.
- Gabriëls RY, van Heijst LE, Hooghiemstra WTR, van der Waaij AM, Kats-Ugurlu G, Karrenbeld A, Robinson DJ, et al. Detection of Early Esophageal Neoplastic Barrett Lesions with Quantified Fluorescence Molecular Endoscopy Using Cetuximab-800CW. J Nucl Med. 2023 May;64(5):803-808.